
At American Endovascular, we prevent more than 80% of amputations in patients who were told there was no other option. No patient should undergo amputation without seeing us first. In this case overview, Dr. Kevin Herman treats a male patient who was at risk of losing a limb due to an infection.
Consultation – History
47-year-old male who developed a severe soft tissue infection on the dorsum of his foot with exposed tendons (right).
He was on vacation in Las Vegas at the time and he was told he would need to have his leg amputated.
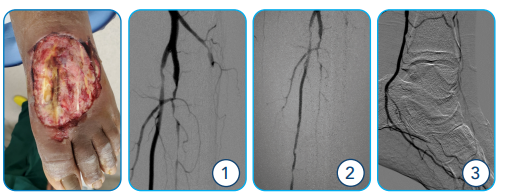
ABOVE (Far Left): Initial Clinical Image of Patient’s Left Foot (1-3): Initial Angiogram reveals occluded AT down to the ankle and multi-focal PT and peroneal artery stenosis.
PMHx:
- DM (not well controlled)
- HTN
- NON-SMOKER
Medications:
- Atorvastatin
- Amlodipine
- Lantus
- Nateglinide
- (Not on anti-plt therapy)
NOTE: At the time of the initial consult, the exact medications were unknown.
Initial Plan and Treatment
- Blood work
- Arterial imaging
- Add anti-plt therapy
- Angiogram and intervention based on the clinical picture, patient history, and arterial imaging
- Try to restore blood flow to as many blood vessels as possible
Initial Findings
- Initial angiogram (images 1-3) shows severe stenotic diffuse disease of all three blood arteries below the knee and specifically no blood flow to the top of the foot at the site of the wound.
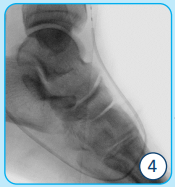
IMAGES 4-5:
Intraprocedural Fluoroscopic Images show the balloon across the pedal loop in both AP and lateral projections.
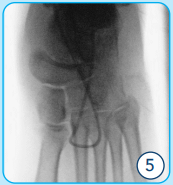
BELOW (6-8):
Final Angiograms demonstrate a patent plantar pedal loop with good flow to the dorsum of the foot via the AT to the location of the wound.
(9-10):
Post Intervention healing had progressed nicely but stalled. New SFA disease warranted a second intervention.
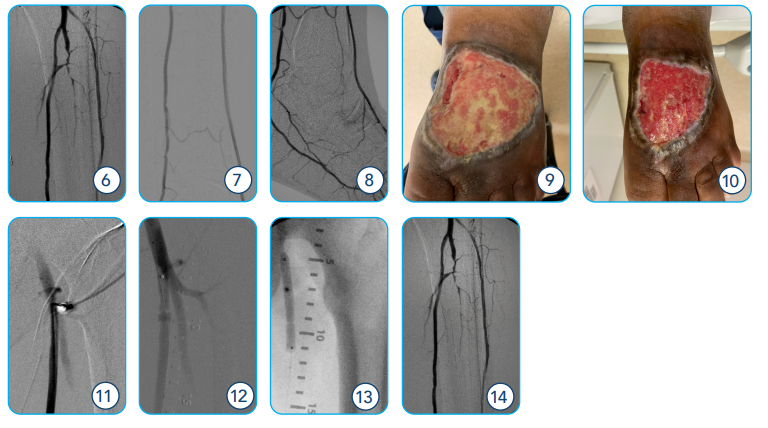
IMAGE 11: Initial Angiogram at Procedure 1 – angiographic images from the first procedure show no proximal SFA disease.
IMAGE 12-13: Angiographic Image at Second Procedure now demonstrates a new SFA lesion treated with balloon angioplasty.
IMAGE 14: Second Intervention shows final angiogram with improved blood flow in the tibial vasculature.
Discussion
- A team approach is key – American Endovascular was in constant communication with the patient’s podiatrist as well as the wound care specialists and home care agency.
- Patient and family both need to be on board with the treatment plan and understand that results are not immediate and that healing takes time – manage expectations.
- Close wound care follow-up is essential.
- Good photographic images of wound – pictures are worth a thousand words for comparison.

ABOVE: Clinical Images after Re-intervention at 6 months (left) and 9 months (right); the wound is almost completely closed; no skin graft needed.
Breakthrough, Non-surgical Limb Saving Treatments Performed in a Fully Equipped Outpatient Center
We believe in the “Toe and Flow” collaboration of care.
Podiatrists treat the toe; we treat the flow.
After restoring blood flow, even in the most complex cases, we collaborate with referring doctors to ensure all patients are returned to their podiatrists for continued treatment.
Highly Trained, Board Certified Endovascular Specialists
Kevin Herman, MD – Interventional Radiologist
A leading authority on PAD and CLI, Dr. Herman graduated from UMDNJ Medical School and completed a fellowship in vascular and interventional radiology at Albert Einstein College of Medicine, Montefiore Health System, Bronx, New York City. He spearheads multiple clinical trials in endovascular medicine, helping evaluate devices and drug therapies for peripheral artery disease. In addition to NJ Endovascular, he also serves as Medical Director of Advanced Interventional & Vascular Services, LLP.
Related Blogs & Videos
Learn more about vascular health, prevention, and care for Peripheral Artery Disease.






Request an Appointment at your nearest American Endovascular affiliated center.