
It’s the 21st Century. Why Are There Still So Many Amputations?
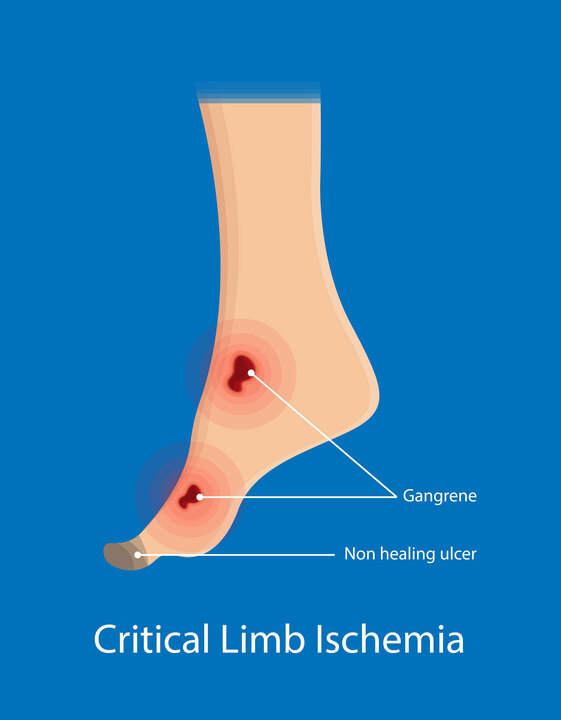
Amputation—the complete or partial removal of a limb—is the most conventional and common approach to treating severe CLI, particularly for older individuals. Critical limb ischemia (CLI) is the most severe form of peripheral artery disease (PAD), causing leg pain at rest, poorly healing foot wounds, or gangrene. As recently as 2017, 70% of CLI patients received amputation before any intervention. Unfortunately, after amputation, most patients deteriorate rapidly. According to a recent study on amputation for chronic CLI:
- The mortality rate is 44% one year after amputation
- 66% mortality rate three years after amputation
- 85% mortality five years after amputation
Patients with severe CLI deserve better. That’s why the American Endovascular affiliated team of physicians is doing something about it. Our medical professionals aim to prevent amputations and save limbs through minimally invasive treatment options, helping patients enjoy longer, healthier, and happier lives.
Their track record speaks for itself. The American Endovascular affiliated team of physicians have been able to restore blood flow and salvage treated limbs for patients that were told they needed a major amputation.
How Amputation Prevention Can Help Treat CLI and Salvage Limbs
American Endovascular’s affiliated physicians provide patients with the most up-to-date minimally invasive-image guided treatment options to save limbs and prolong life. Endovascular treatment is the least invasive way to restore blood flow to limbs. Here’s how some endovascular procedures work:
- A catheter (thin plastic tube) is inserted into the artery, without surgery, through a small nick in the skin at the groin or in the foot. The nick is so small there is not even an incision to heal.
- A catheter is threaded to the area of narrowing and disease, which has been affected by plaque build-up.
- Specialized catheters open the blocked arteries by removing or destroying plaque (called atherectomy) or displacing and disrupting it with a balloon that is inflated briefly. Atherectomy may include a variety of additional advanced tools such as laser, as well as orbital and rotational atherectomy. The opening of arteries with a balloon catheter is called angioplasty.
- A variety of additional state-of-the-art methods may be utilized and inserted to keep the artery open, including drug delivery systems, stents, covered stents, drug-eluting stents (DES), and drug-covered stents (DCS).

How Does the Pedal Loop Technique Help with Limb Salvage?
At American Endovascular, our affiliated physicians are also skilled in performing the Pedal Loop Technique to prevent amputations for patients with PAD and CLI. Pedal loop interventions that can help with limb salvage and limb preservation in patients with non-healing wounds due to diabetes, chronic kidney disease, and other conditions. The pedal loop consists of arteries in the foot that are responsible for supplying blood to the toes and the heel.
Patients with blockages in the pedal loop due to diabetes and other conditions can develop wounds, ulcers, or gangrene that don’t heal without restoring blood flow. While not every person needs a pedal loop intervention, there are certainly individuals for whom, when the wounds don’t heal, this type of intervention is extremely important in order to provide the best results. Most notably, it is a procedure that not many interventionalists are comfortable performing due to the small diameter of these arteries.

Why Choose American Endovascular for Amputation Prevention?
American Endovascular affiliated physicians save the limbs that others can’t. Our affiliated team of vascular specialists is at the forefront of the battle to prolong life by preventing amputations. They accomplish this by using the most advanced minimally invasive-image guided endovascular treatment options available anywhere, to save limbs and save lives. Below are more reasons why our affiliated physicians are the ‘best of the best.”
- The physicians affiliated with American Endovascular are recognized worldwide as innovators in the field of complex lower extremity PAD and CLI treatment.
- They have demonstrated success in restoring optimal blood flow by targeting blocked arteries in the ankle and feet using specialized techniques and tools.
- They can treat patients who have been told by other doctors that they have “no other options” than amputation..
- They specialize in treating the small, extremely difficult blocked arteries in the foot and toes that others do not attempt to treat.
- They have access to clinical trials that others do not.
Our Vascular Specialists
Our affiliated vascular specialists perform amputation prevention procedures for patients in New York and New Jersey. Their goal is to provide patients with the highest level of care, so they can prevent PAD from progressing further and save the lives of their patients.







What Our Patients Are Saying









")














































Recent Blogs & Videos
Learn more about vascular health, prevention, and care for Peripheral Artery Disease.






Request an Appointment at your nearest American Endovascular affiliated center.